Modern instrumentation for cervical stabilization in pediatric patients
For years, the pars and pedicle have been the primary fixation points in cervical spine-stabilization procedures in pediatric patients. Unfortunately, there are well-known downsides to the use of C2 pars/pedicle screws, including proximity to the vertebral artery and heightened risk of serious injury. In some cases, a patient’s anatomical anomalies make it impossible to attach a screw to these sections of the vertebrae.
Orthopedic surgeon Daniel Hedequist, MD, described these shortcomings in an article published in the Journal of the American Academy of Orthopaedic Surgeons in 2016 and suggested translaminar screws as a viable alternative. Translaminar screws have been shown to provide a biomechanically strong anchor and are a reasonable fixation option in even the youngest patients with cervical spine instability.
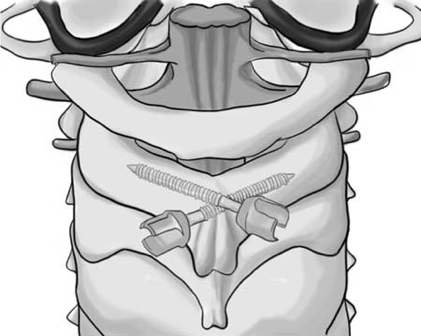 Bilateral C2 translaminar screws
Bilateral C2 translaminar screwsBecause translaminar screws are placed on the opposite side of the spinous process, using translaminar screws avoids the risk of injuring the vertebral artery. Further, the majority of children over the age of 2 have anatomies appropriate for translaminar screw fixation. Because the instrumentation has not been well investigated in children, however, translaminar C2 screws have historically been used primarily in adult patients and are underutilized by pediatric surgeons.
Investigating translaminar screw utilization in children
In order to better understand the safety and efficacy of translaminar C2 screw fixation for pediatric patients, we searched surgical records of cervical spinal fusion surgeries that encompassed C2 from 2007 to 2017 in the Boston Children’s Hospital orthopedic database. Our analysis included types of C2 screw fixation, patient age, diagnosis, fusion level and procedure details.
In total, 23 patients met our inclusion criteria. Patients ranged in age from 5.2 to 17.8 years old, with a mean age of 12.6 years. Diagnoses included instability related to skeletal dysplasia, os odontoideum, congenital deformities, basilar invaginations, cervical spine tumors and spinal fracture. In the majority of cases, the decision to use translaminar screws was made preoperatively due to distortions in the patients’ anatomy that made it impossible to use pars screws.
In three cases, C2 translaminar screws were used as a salvage technique. In two cases, the patients’ suffered vertebral artery injury during dissection with distorted anatomy. In one other case, the vertebral artery intersected a tumor and was intentionally sacrificed. In six cases, no reason for this choice of screw was documented.
A safe and solid option for pediatric cervical spinal fusion surgery
There were no screw-related intraoperative or postoperative complications and no neurological injuries in any of the surgeries using C2 translaminar screws. All patients demonstrated clinical union or healing.
The results of this case series demonstrate that C2 translaminar screw fixation may be performed safely and serves as a solid base for fusions involving the upper cervical spine. We recommend pediatric orthopedic surgeons consider C2 translaminar screw fixation as a safe, effective technique for their pediatric patients undergoing cervical spinal fusion surgery.
Articles referenced
Yang BW, Glotzbecker MP, Troy M, Proctor MR, Hresko MT, Hedequist DJ. C2 Translaminar Screw Fixation in Children. J Pediatr Ortho. 2018 Jul; 38(6):e312-e317.
Hedequist DJ, Emans JB. Cervical Spine Instrumentation in Children. J Am Acad Orthop Surg. 2016 Jun; 24(6):370-8.
Related articles
Brockmeyer DL, Sivakumar W, Mazur MD, Sayama CM, Goldstein HE, Lew SM, Hankinson TC, Anderson RCE, Jea A, Aldana PR, Proctor M, Hedequist D, Riva-Cambrin JK; Pediatric Craniocervical Society. Identifying Factors Predictive of Atlantoaxial Fusion Failure in Pediatric Patients: Lessons Learned From a Retrospective Pediatric Craniocervical Society Study.Spine (Phila Pa 1976). 2018 Jun 1;43(11):754-760.
Porter DA, Glotzbecker MP, Timothy Hresko M, Hedequist DJ. Deep Surgical Site Infections Following Pediatric Cervical Spine Surgery. J Pediatr Orthop. 2017 Dec;37(8):553-556.
Tobert DG, Glotzbecker MP, Hresko MT, Karlin LI, Proctor MR, Emans JB, Miller PE, Hedequist DJ. Efficacy of Intraoperative Neurophysiologic Monitoring for Pediatric Cervical Spine Surgery.Spine (Phila Pa 1976). 2017 Jul 1;42(13):974-978.
Murphy RF, Glotzbecker MP, Hresko MT, Hedequist D. Allograft Bone Use in Pediatric Subaxial Cervical Spine Fusions. J Pediatr Orthop. 2017 Mar;37(2):e140-e144.
Abd-El-Barr MM, Snyder BD, Emans JB, Proctor MR, Hedequist D. Combined preoperative traction with instrumented posterior occipitocervical fusion for severe ventral brainstem compression secondary to displaced os odontoideum: technical report of 2 cases. J Neurosurg Pediatr. 2016 Dec;25(6):724-729. Epub 2016 Aug 26
Helenius IJ, Sponseller PD, Mackenzie W, Odent T, Dormans JP, Asghar J, Rathjen K, Pahys JM, Miyanji F, Hedequist D, Phillips JH. Outcomes of Spinal Fusion for Cervical Kyphosis in Children with Neurofibromatosis.J Bone Joint Surg Am. 2016 Nov 2;98(21):e95.
Helenius I, Crawford H, Sponseller PD, Odent T, Bernstein RM, Stans AA, Hedequist D, Phillips JH. Rigid fixation improves outcomes of spinal fusion for C1-C2 instability in children with skeletal dysplasias. J Bone Joint Surg Am. 2015 Feb 4;97(3):232-40.
Hedequist D. Modern instrumentation of the pediatric occiput and upper cervical spine: review article. HSS J. 2015 Feb;11(1):9-14. Epub 2014 Aug 12. Review.
Hedequist DJ. Modern posterior screw techniques in the pediatric cervical spine.
World J Orthop. 2014 Apr 18;5(2):94-9. eCollection 2014 Apr 18. Review.
Glotzbecker MP, Wasser AM, Hresko MT, Karlin LI, Emans JB, Hedequist DJ. Efficacy of nonfusion treatment for subacute and chronic atlanto-axial rotatory fixation in children. J Pediatr Orthop. 2014 Jul-Aug;34(5):490-5.
Zenonos G, Jamil O, Governale LS, Jernigan S, Hedequist D, Proctor MR. Surgical treatment for primary spinal aneurysmal bone cysts: experience from Children's Hospital Boston. J Neurosurg Pediatr. 2012 Mar;9(3):305-15.
Hedequist D, Proctor M, Hresko T. Lateral mass screw fixation in children.
J Child Orthop. 2010 Jun;4(3):197-201. Epub 2010 Mar 19.
Hedequist D, Bekelis K, Emans J, Proctor MR. Single stage reduction and stabilization of basilar invagination after failed prior fusion surgery in children with Down's syndrome. Spine (Phila Pa 1976). 2010 Feb 15;35(4):E128-33.
Hedequist D, Proctor M. Screw fixation to C2 in children: a case series and technical report. J Pediatr Orthop. 2009 Jan-Feb;29(1):21-5.
Hedequist D, Hresko T, Proctor M. Modern cervical spine instrumentation in children. Spine (Phila Pa 1976). 2008 Feb 15;33(4):379-83.